Recently we have had a couple of cases of nail penetration of the foot which highlighted the potential risks of this injury and the need for immediate correct treatment. Excellent knowledge of the anatomy of the foot is crucial to understand where a penetrating object can reach and why the consequences can be so serious.
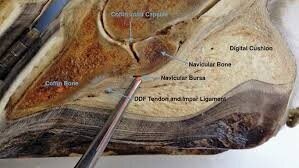
Sagittal section through the hoof, the pointer is marking the position of the navicular bursa.
As you can see from the image above, a nail penetration in the direction of the pointer will pass through the digital cushion, the deep flexor tendon and into the navicular bursa. Inevitably the nail will introduce dirt and bacteria into these sensitive areas. If navicular bursal penetration is not treated immediately, the structure will become chronically infected and ultimately the horse would have to be euthanased on welfare grounds. So accurate evaluation of the injury is vital to ensure that the correct treatment options are employed. If possible, we take x-ray images of the foot with the nail in situ so that we can appreciate its trajectory. Often, however, owners have already removed the nail prior to calling the vet. In these cases, after thoroughly cleaning the sole, we attempt to introduce a metal probe into the hole left by the nail so that we can see that on our x-ray instead. We can also inject a radio-opaque dye into the hole which shows up on x-rays and helps us assess the extent of the penetration. MRI is another option, if readily available, to evaluate which structures have been compromised

Probe inserted into nail penetration tract .
The radiographic image above is from one of our recent cases; it shows the nail will have penetrated through the digital cushion and the deep flexor tendon and will therefore have introduced bacteria close to the navicular bursa.This horse was extremely lame. The foot was prepared with a rasp and hoof knife so that all loose tissue was removed. The whole foot was then dressed in iodine-soaked bandages for an hour prior to being taken to surgery. Under general anaesthesia the penetrating tract through the frog was explored and enlarged so that the digital cushion and deep flexor tendon could be flushed with sterile saline under high pressure. The arthroscope was then introduced via a portal in the pastern region, down into the navicular bursa. This structure was explored for signs of penetration, which fortunately had not occurred in this case, and was then flushed using an exit portal. Antibiotics were then deposited into the bursa. If there had been penetration of the bursa, then flush fluids would have found there way out through the frog wound, this obviously didn’t occur in this case. At the end of the surgical procedure the foot and the lower limb were dressed very carefully with sterile protective dressings. These cases are put on high doses of strong broad-spectrum antibiotics for a minimum of five days. With this case the recovery has been uneventful and following two weeks of dressings, the foot was then fitted with a shoe and hospital plate which allows us access to the frog region to regularly inspect the healing frog wound.

Shoe fitted with a hospital plate to allow access to the healing penetration wound in the frog.
The second of the recent cases involved a nail penetration in the cleft of the frog just in front of the site of attachment of the deep flexor tendon to the pedal bone. The nail had been removed by the owner and so after thorough cleansing, a probe was introduced into the hole to establish the trajectory . Luckily although it went down to bone, it was heading forwards and so missed the tendon, but only just! With this case, the hole was opened-up to aid flushing and to provide a drainage route for any pus. The foot was poulticed for two days then dressed with iodine soaked bandages. This horse was put on the same broad-spectrum combination of antibiotics and no pain relief was allowed so that the horse’s true level of comfort was known. His recovery was straightforward. It is absolutely crucial to make sure that these patients have been vaccinated against tetanus as they would be nailed-on (excuse the pun) to get it otherwise. If in doubt, tetanus antitoxin should be given to provide immediate cover.
So in summary, if your horse is unlucky enough to suffer from a nail penetration of the foot, call us straight away and try and resist the temptation to remove the nail!